
Obese Patients and Worse Care
By Zewen Tan September 30, 2016
Obesity in America has been a steadily expanding issue over the past few decades. The rate today is at over thirty five percent; that is almost two in five people whose body mass index is over 30+ (1 Overweight). Another 15 million Americans are morbidly obese with a BMI of over 40+ (4 Sturm). Studies have shown that multiple health issues and diseases arise as a direct result of having excessive body fat, including: heart disease and stroke, high blood pressure, diabetes, gallbladder disease, osteoarthritis, and breathing problems (3 Health). Unfortunately, even with medical research and procedures advancing at a rate never before seen, the healthcare system is still not ready for proper treatment of the growing population or obese patients.
There are numerous cases of physicians overlooking serious medical conditions in patients simply because of their weight. Patty Nece, a middle aged woman in Virginia, went to her orthopedist due to pain in her hip. The doctor remarked about how a diet was needed before diagnosing the issue as simply “obesity pain”. After relaying the experience to her internist, Mrs. Nece found that she had progressive scoliosis, a health case unrelated to obesity. Another woman who went to the local urgent care center in Washington for breathing trouble was told that the only thing wrong was that she was fat. After seeing a specialist at Georgetown University, blood clots were discovered in her lungs. This pattern of inequality has led to a study in the Texas Medical Center in Houston, where it was found that while “physicians prescribed more tests for heavier patients… they simultaneously indicated that they would spend less time with them” (5 Hebl). Furthermore, the physicians described the obese patients to be “more annoying” and “a greater waste of their time”.
The problem does not end with the physicians. The tests prescribed by the doctors require special equipment such as CT and MRI scanners. Most models usually support between 350-450 pounds, but that is often not enough for morbidly obese patients. Larger scanners do exist and are still manufactured, but they are not readily available. A study found that a measly 10% of US hospitals had these scanners (6 Ginde). Some doctors may simply give up after this point, but others have tried to send patients to zoos or veterinary schools for a scan. This decision is not optimal, both because of animal-human incompatibilities and patient shame.
Another issue arises when prescribing medication. Dosages are based on a set standard of body sizes or surface areas. These measurements do not scale up linearly because body components such as muscle, bone, or fat does not increase linearly with weight (7 Baerdemaeker). Mistakes in this aspect may cause procedural complications or even death, which is behind the refusals of some doctors to operate on patients. A decrease in rating means a reduction in reimbursements by Medicare, which after trickling down the healthcare system, results in penalties for the doctors. A common practice among hospitals to avoid these issues is to pick an arbitrary BMI cutoff for surgery. This bodes poorly for those who are just above the cut, but still grouped with those at high risk.
The healthcare system today still has a ways to go in order to ensure the proper treatment of obese patients. There needs to not only be a massive overhaul in the equipment and policies of hospitals, but a complete paradigm shift in how we view logistically challenging patients. After all, they have health issues just like the rest of us.
Obesity in America has been a steadily expanding issue over the past few decades. The rate today is at over thirty five percent; that is almost two in five people whose body mass index is over 30+ (1 Overweight). Another 15 million Americans are morbidly obese with a BMI of over 40+ (4 Sturm). Studies have shown that multiple health issues and diseases arise as a direct result of having excessive body fat, including: heart disease and stroke, high blood pressure, diabetes, gallbladder disease, osteoarthritis, and breathing problems (3 Health). Unfortunately, even with medical research and procedures advancing at a rate never before seen, the healthcare system is still not ready for proper treatment of the growing population or obese patients.
There are numerous cases of physicians overlooking serious medical conditions in patients simply because of their weight. Patty Nece, a middle aged woman in Virginia, went to her orthopedist due to pain in her hip. The doctor remarked about how a diet was needed before diagnosing the issue as simply “obesity pain”. After relaying the experience to her internist, Mrs. Nece found that she had progressive scoliosis, a health case unrelated to obesity. Another woman who went to the local urgent care center in Washington for breathing trouble was told that the only thing wrong was that she was fat. After seeing a specialist at Georgetown University, blood clots were discovered in her lungs. This pattern of inequality has led to a study in the Texas Medical Center in Houston, where it was found that while “physicians prescribed more tests for heavier patients… they simultaneously indicated that they would spend less time with them” (5 Hebl). Furthermore, the physicians described the obese patients to be “more annoying” and “a greater waste of their time”.
The problem does not end with the physicians. The tests prescribed by the doctors require special equipment such as CT and MRI scanners. Most models usually support between 350-450 pounds, but that is often not enough for morbidly obese patients. Larger scanners do exist and are still manufactured, but they are not readily available. A study found that a measly 10% of US hospitals had these scanners (6 Ginde). Some doctors may simply give up after this point, but others have tried to send patients to zoos or veterinary schools for a scan. This decision is not optimal, both because of animal-human incompatibilities and patient shame.
Another issue arises when prescribing medication. Dosages are based on a set standard of body sizes or surface areas. These measurements do not scale up linearly because body components such as muscle, bone, or fat does not increase linearly with weight (7 Baerdemaeker). Mistakes in this aspect may cause procedural complications or even death, which is behind the refusals of some doctors to operate on patients. A decrease in rating means a reduction in reimbursements by Medicare, which after trickling down the healthcare system, results in penalties for the doctors. A common practice among hospitals to avoid these issues is to pick an arbitrary BMI cutoff for surgery. This bodes poorly for those who are just above the cut, but still grouped with those at high risk.
The healthcare system today still has a ways to go in order to ensure the proper treatment of obese patients. There needs to not only be a massive overhaul in the equipment and policies of hospitals, but a complete paradigm shift in how we view logistically challenging patients. After all, they have health issues just like the rest of us.
| Bibliography |
EpiPen Affordability: The Cost of Saving Lives
By Anneliese Lapides October 3, 2016
According to the Wall Street Journal, about 3.6 million people were prescribed EpiPens in America in 20151 in order to combat allergic reactions to stings and foods such as peanuts. EpiPens contain the hormone epinephrine, a manmade version of adrenaline. Epinephrine acts against allergic reactions when injected into the body by constricting blood vessels, or making them smaller2. This constricting of the blood vessels increases blood pressure and relaxes the muscles of the lungs in order to restore breathing. This also increases heart rate and reduces swelling caused by the allergic reaction. Because EpiPens provide crucial medication to so many people of all ages across the country with harmful allergies, it is important that they be affordable. The recent controversy surrounding EpiPens is the expensive cost. Mylan, one of the largest international pharmaceutical companies, has increased the price of EpiPens over the past decade due to upgrades in the model of the medicine-delivering contraption. However, some argue that the “new” EpiPen is hardly so different from the EpiPen that exponentially less expensive nine years ago. While pharmaceutical company pricing is not a new issue, the controversy over the price of the EpiPen is making recent headlines due to its importance in the lives of so many Americans. This demographic includes children, who constantly face the risk of encountering their allergen in their everyday lives.
The CEO of Mylan, Heather Bresch, must defend the company’s reason for the increase in the price of EpiPen in front of Congress. In a New York Times interview, her rebuttal to the controversy over the high cost of the EpiPen was “‘I am running a business.’”3 How much has Mylan increased the price of the EpiPen? In 2007, the device cost around $100. Now, the device costs over $600; this is a 400 percent increase in price over the past nine years4. The medicine inside of the contraption does have an expiration date, which requires up to an additional $500 to refill4.
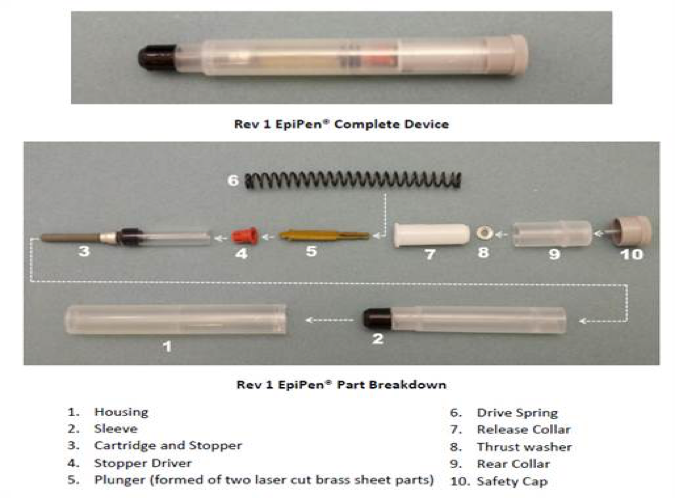
Mylan has connected the large price increase of the EpiPen to upgrades made in the structure of the device. Two versions of the device were compared by PA Consulting Group, a technology consulting firm in the UK5. The EpiPen pictured below is one with a 2009 expiration date. Photo: nbcnew.com5.
According to the Wall Street Journal, about 3.6 million people were prescribed EpiPens in America in 20151 in order to combat allergic reactions to stings and foods such as peanuts. EpiPens contain the hormone epinephrine, a manmade version of adrenaline. Epinephrine acts against allergic reactions when injected into the body by constricting blood vessels, or making them smaller2. This constricting of the blood vessels increases blood pressure and relaxes the muscles of the lungs in order to restore breathing. This also increases heart rate and reduces swelling caused by the allergic reaction. Because EpiPens provide crucial medication to so many people of all ages across the country with harmful allergies, it is important that they be affordable. The recent controversy surrounding EpiPens is the expensive cost. Mylan, one of the largest international pharmaceutical companies, has increased the price of EpiPens over the past decade due to upgrades in the model of the medicine-delivering contraption. However, some argue that the “new” EpiPen is hardly so different from the EpiPen that exponentially less expensive nine years ago. While pharmaceutical company pricing is not a new issue, the controversy over the price of the EpiPen is making recent headlines due to its importance in the lives of so many Americans. This demographic includes children, who constantly face the risk of encountering their allergen in their everyday lives.
The CEO of Mylan, Heather Bresch, must defend the company’s reason for the increase in the price of EpiPen in front of Congress. In a New York Times interview, her rebuttal to the controversy over the high cost of the EpiPen was “‘I am running a business.’”3 How much has Mylan increased the price of the EpiPen? In 2007, the device cost around $100. Now, the device costs over $600; this is a 400 percent increase in price over the past nine years4. The medicine inside of the contraption does have an expiration date, which requires up to an additional $500 to refill4.
Mylan has connected the large price increase of the EpiPen to upgrades made in the structure of the device. Two versions of the device were compared by PA Consulting Group, a technology consulting firm in the UK5. The EpiPen pictured below is one with a 2009 expiration date. Photo: nbcnew.com5.
The second EpiPen, pictured below, has a 2015 expiration date and replaces some pieces while also including new, additional pieces. Photo: nbcnews.com5.
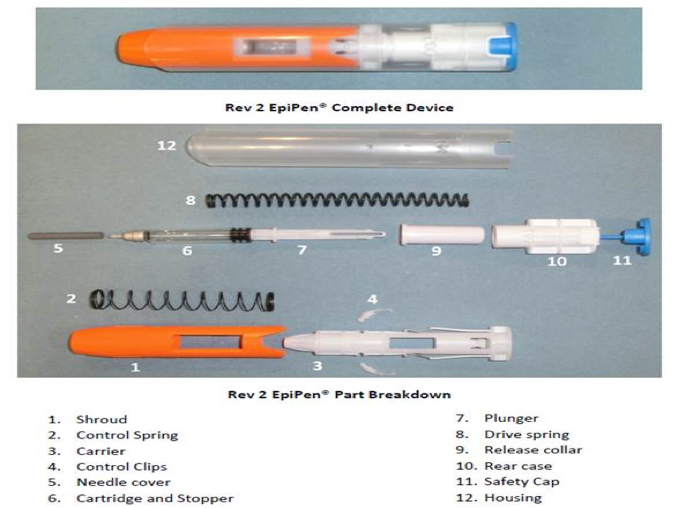
In conclusion of their investigation, the head of the medical technology branch of PA Consulting Group stated: “‘It’s the same core device that’s been in use for some time.’”5 This comparison of the two models, the former over $500 less than the latter, is an example of the overall function and practicality of the device is the same in both devices.
So we ask ourselves, if both models perform the same function in the same general manner, then why should the new model be so much more expensive? For families with children who have allergies, it is important that they are able to afford EpiPens in order to provide proper medical care if a life-threatening allergic reaction were to occur. While EpiPens are covered by most insurance companies, some Americans do not have insurance or they have providers who do not cover the medicine-delivering device or epinephrine refills. Affordability of medicine is already a greatly argued problem in our country, and EpiPens are no exception. It is incredibly likely that most people know at least one person who needs an EpiPen. The necessity of this product in so many peoples’ lives should be taken into consideration when discussing its price in order for this medicine to reach the people who need it and, in turn, save lives.
So we ask ourselves, if both models perform the same function in the same general manner, then why should the new model be so much more expensive? For families with children who have allergies, it is important that they are able to afford EpiPens in order to provide proper medical care if a life-threatening allergic reaction were to occur. While EpiPens are covered by most insurance companies, some Americans do not have insurance or they have providers who do not cover the medicine-delivering device or epinephrine refills. Affordability of medicine is already a greatly argued problem in our country, and EpiPens are no exception. It is incredibly likely that most people know at least one person who needs an EpiPen. The necessity of this product in so many peoples’ lives should be taken into consideration when discussing its price in order for this medicine to reach the people who need it and, in turn, save lives.
| Bibliography |
Resistance to Drugs Effecting Us All
By Meghan Goddard October 2, 2016
Often a topic haunting the medical world and instilling fear in families is the idea of our increase resistance to drugs. The future of resistance has been an alarm to the medical realm for years, but is quickly becoming prevalent now. On September 21, 2016, the United Nations met in New York to discuss the worsening issue of antimicrobial resistance and its risk to humans, animals, and agriculture. This is a current issue occurring in countries of all stages of development and goes beyond hospitals to farms that effects animals and humans. Resistance is built overtime through abuse or misuse of different antibiotics seen in agricultural treatments to crops and over prescription or vaccination in hospitals. In the agricultural world, different antimicrobials are used to protect us against harmful microorganisms, but in the process over exposes us. Deposits from these antibiotics can travel through the soil into the crops that we consume and the water we drink, proving this is an issue effecting the wellbeing of all (Robertson).
At the conference, the general assembly agreed each nation will develop an action plan on ways to cut back on antimicrobials in agriculture and decrease abuse of antibiotics in hospitals, based on a plan put together by the World Health Organization, the Food and Agriculture Organization, and the World Organization for Animal Health (Robertson).
Our resistance to medications against these microbes and harmful species increases chances of chronic infections and diminishes our ability to prevent these illnesses. The widespread idea of the dangers of resistance has come to many people’s attention with regards to flu shots. Recent studies have supported the claim that the annual flu shot is decreasing its benefits as a vaccine. The Center for Disease Control and Prevention (CDC) have already recommended physicians and parents halt the use of the nasal mist method of the influenza vaccine, as it has shown to be less to completely ineffective, a struggle for many patients and children. Even with the injection the repeated use of the vaccine, like the antimicrobials, can lead to a resistance by our bodies producing less and less antibodies produced each successive year we receive the vaccine. This presence a major conflict in that the United States is a huge proponent of promoting yearly flu shots, as seen in advertisements every time you step into a waiting room, local drug store, or school. These new studies contradict this nationwide support, leaving patients and parents hesitant. However, because the vaccination fights against up to four different strains of the virus, it is still helpful against at least one or two strains each year. The CDC reports this vaccine still decreases the chances of getting influenza for that given year by 70 to 90%, despite other health institutes claiming closer to 50% (Branswell, “Science of Flu Shots”). Either way, getting the injection version of the vaccine still prevents, at some extent, the risk of that awful winter flu we all rather avoid.
The rising issue of resistance is prevalent in widespread situations, like antimicrobials, and even effecting the common flu, and recently has been seen in more serious illnesses like sexually transmitted infections. Azithromycin and ceftriaxone, for example, are two drugs used to treat gonorrhea, yet the CDC has recently found many cases in Hawaii where the bacteria involved with the STI has been opposing treatments. A CDC director, Dr. Jonathan Mermin, warns that the bacteria has resisted many drugs before and this may be the last effort, putting hundreds of thousands of Americans at risk each year. So far these patients have been treated with repeat doses, but scientists fear these drugs will fail as new antibiotics are years away for medical use (Branswell, “Gonorrhea”).
The more resistance our immune systems build against medications and the more viruses or bacteria are able to resist our advanced medications, the more panic surfaces. Nevertheless, so do advances in research. To think of how far research has come to even have a vaccine for illnesses like influenza or HPV, or drugs to treat gonorrhea, is incredible. Although it may take a few years, a new drug for gonorrhea is on its way to the market, so we can have some trust in our advancements in research year after year (Branswell, “Gonnorhea”). Even though prevention of influenza decrease year after year, research continues to move forward, and I have hope they will develop a flu shot to keep up with the changing strands and decrease of antibodies. As Branswell states, “some protection is better than none” (Branswell, “Science of Flu Shots”). As a huge proponent of vaccines, I believe it is important to use what little preventions we have set in place. What is one shot for decreasing your risk of getting the flu by at least 50%, or a few extra doses of medications to treat a painful STI. However, it is also important to keep up with research and physicians’ or the CDC’s recommendations each year. In terms of antimicrobials, putting the pressure to reduce resistance entirely on agriculture creates a dangerous loop. To use less antimicrobials in agriculture means possible increase in spread of dangerous microorganisms that are now not being killed off. As Robertson explained, any reduction may help, failing to cut back on the overuse of antibiotics and pesticides will lead to threatening consequences (Robertson). It is important to follow as the UN forms a plan to improve the issue, to keep up with our vaccines, and to do the best to protect ourselves by staying updated with the evolving medical world.
Often a topic haunting the medical world and instilling fear in families is the idea of our increase resistance to drugs. The future of resistance has been an alarm to the medical realm for years, but is quickly becoming prevalent now. On September 21, 2016, the United Nations met in New York to discuss the worsening issue of antimicrobial resistance and its risk to humans, animals, and agriculture. This is a current issue occurring in countries of all stages of development and goes beyond hospitals to farms that effects animals and humans. Resistance is built overtime through abuse or misuse of different antibiotics seen in agricultural treatments to crops and over prescription or vaccination in hospitals. In the agricultural world, different antimicrobials are used to protect us against harmful microorganisms, but in the process over exposes us. Deposits from these antibiotics can travel through the soil into the crops that we consume and the water we drink, proving this is an issue effecting the wellbeing of all (Robertson).
At the conference, the general assembly agreed each nation will develop an action plan on ways to cut back on antimicrobials in agriculture and decrease abuse of antibiotics in hospitals, based on a plan put together by the World Health Organization, the Food and Agriculture Organization, and the World Organization for Animal Health (Robertson).
Our resistance to medications against these microbes and harmful species increases chances of chronic infections and diminishes our ability to prevent these illnesses. The widespread idea of the dangers of resistance has come to many people’s attention with regards to flu shots. Recent studies have supported the claim that the annual flu shot is decreasing its benefits as a vaccine. The Center for Disease Control and Prevention (CDC) have already recommended physicians and parents halt the use of the nasal mist method of the influenza vaccine, as it has shown to be less to completely ineffective, a struggle for many patients and children. Even with the injection the repeated use of the vaccine, like the antimicrobials, can lead to a resistance by our bodies producing less and less antibodies produced each successive year we receive the vaccine. This presence a major conflict in that the United States is a huge proponent of promoting yearly flu shots, as seen in advertisements every time you step into a waiting room, local drug store, or school. These new studies contradict this nationwide support, leaving patients and parents hesitant. However, because the vaccination fights against up to four different strains of the virus, it is still helpful against at least one or two strains each year. The CDC reports this vaccine still decreases the chances of getting influenza for that given year by 70 to 90%, despite other health institutes claiming closer to 50% (Branswell, “Science of Flu Shots”). Either way, getting the injection version of the vaccine still prevents, at some extent, the risk of that awful winter flu we all rather avoid.
The rising issue of resistance is prevalent in widespread situations, like antimicrobials, and even effecting the common flu, and recently has been seen in more serious illnesses like sexually transmitted infections. Azithromycin and ceftriaxone, for example, are two drugs used to treat gonorrhea, yet the CDC has recently found many cases in Hawaii where the bacteria involved with the STI has been opposing treatments. A CDC director, Dr. Jonathan Mermin, warns that the bacteria has resisted many drugs before and this may be the last effort, putting hundreds of thousands of Americans at risk each year. So far these patients have been treated with repeat doses, but scientists fear these drugs will fail as new antibiotics are years away for medical use (Branswell, “Gonorrhea”).
The more resistance our immune systems build against medications and the more viruses or bacteria are able to resist our advanced medications, the more panic surfaces. Nevertheless, so do advances in research. To think of how far research has come to even have a vaccine for illnesses like influenza or HPV, or drugs to treat gonorrhea, is incredible. Although it may take a few years, a new drug for gonorrhea is on its way to the market, so we can have some trust in our advancements in research year after year (Branswell, “Gonnorhea”). Even though prevention of influenza decrease year after year, research continues to move forward, and I have hope they will develop a flu shot to keep up with the changing strands and decrease of antibodies. As Branswell states, “some protection is better than none” (Branswell, “Science of Flu Shots”). As a huge proponent of vaccines, I believe it is important to use what little preventions we have set in place. What is one shot for decreasing your risk of getting the flu by at least 50%, or a few extra doses of medications to treat a painful STI. However, it is also important to keep up with research and physicians’ or the CDC’s recommendations each year. In terms of antimicrobials, putting the pressure to reduce resistance entirely on agriculture creates a dangerous loop. To use less antimicrobials in agriculture means possible increase in spread of dangerous microorganisms that are now not being killed off. As Robertson explained, any reduction may help, failing to cut back on the overuse of antibiotics and pesticides will lead to threatening consequences (Robertson). It is important to follow as the UN forms a plan to improve the issue, to keep up with our vaccines, and to do the best to protect ourselves by staying updated with the evolving medical world.
| Bibliography |
HPV |
By Francis Regala October 3, 2016
HPV, or Human Papillomavirus, is a common cancer inducing virus that effects nearly one in every four people, adding up to around 80 million globally. This ability for HPV to spread quickly is attributed to it being able to infect individuals via exposure to bodily fluids. While HPV goes away on its own in most cases, not causing any damage, the few cases in which it doesn’t can serious health problems. Amongst these are genital warts, and even worse, cancer, of which many strains are not permanently treatable.
While HPV isn’t cancer itself, it causes biological changes in humans that can potentially lead to cancer. Examples of such are cervical, anal, and oropharyngeal (mouth and throat) cancer in women, as well as penile, anal, and oropharyngeal cancer in men. Even more problematic is that individuals affected with such conditions may not show symptoms for months or even years after their initial contact with HPV.
Because there is no way to determine whether or not an HPV infection for an individual will be long or short term, the best option is to get vaccinated. While many women are already vaccinated for HPV, as they were the focus of HPV treatment since the release of its vaccine in 2007, men have been seriously neglected up until the last several years for protection against the disease. However, while many people now understand that HPV can affect both men and women, there are many males who are left unvaccinated, while 9000 males are infected every year with cancers that cannot be permanently treated due to HPV. Given this information, it is important for individuals, especially males, to check if they have been vaccinated for HPV and to consult their physicians for future treatment if they have yet to be treated.
HPV, or Human Papillomavirus, is a common cancer inducing virus that effects nearly one in every four people, adding up to around 80 million globally. This ability for HPV to spread quickly is attributed to it being able to infect individuals via exposure to bodily fluids. While HPV goes away on its own in most cases, not causing any damage, the few cases in which it doesn’t can serious health problems. Amongst these are genital warts, and even worse, cancer, of which many strains are not permanently treatable.
While HPV isn’t cancer itself, it causes biological changes in humans that can potentially lead to cancer. Examples of such are cervical, anal, and oropharyngeal (mouth and throat) cancer in women, as well as penile, anal, and oropharyngeal cancer in men. Even more problematic is that individuals affected with such conditions may not show symptoms for months or even years after their initial contact with HPV.
Because there is no way to determine whether or not an HPV infection for an individual will be long or short term, the best option is to get vaccinated. While many women are already vaccinated for HPV, as they were the focus of HPV treatment since the release of its vaccine in 2007, men have been seriously neglected up until the last several years for protection against the disease. However, while many people now understand that HPV can affect both men and women, there are many males who are left unvaccinated, while 9000 males are infected every year with cancers that cannot be permanently treated due to HPV. Given this information, it is important for individuals, especially males, to check if they have been vaccinated for HPV and to consult their physicians for future treatment if they have yet to be treated.
| Bibliography |
Mental Health and the Treatment of Suicide
By Colin Bixler October 3, 2016
This past week here at UConn students observed 1100 flags spread across the lawn in front of the student union, placed in memorial to the average of 1100 college students who commit suicide on college campuses each year. Many took the time to write a message of hope, or one in remembrance of someone whom they had known who committed suicide. It brought it to mind for many people, reminded us that there are people who struggle every day with mental illness, and that there are students like us, who believe they have no other option than to commit suicide.
If one were to stop and talk to the group who were tabling in front of the lawn they would have the opportunity to write their flag, collect a button or a shirt, and maybe pet a dog. But they could also learn a little bit more about the organization behind the event, Active Minds, and its mission to reduce the stigma around mental health. It is generally believed that although an important issue in modern society, there is some sort of disconnect between the people trying to give help and those needing it, partly due to the stigma surrounding admitting to your friends and family that you need help. Regardless, mental health is an issue that general physicians are starting to take more awareness of.
Recently, more and more papers have been published that focused on the ways which primary care physicians, as well as counseling and psychiatry centers, can improve the way in which they approach the issue. Some studies have shown ways to improve the appearance of facilities to make them more friendly, so as to reduce the rates of suicide at in-patient facilities. Others have been published more as advice, based on research, to primary care physicians on how to approach the issue, from simply looking for specific risk factors, to broaching the subject with their patients.
Regardless of who the target audience is, mental health is a topic that needs to be better approached. One study that looked into the medical records of patients who had eventually committed suicide found that “only one third” had spoken to a mental health services center, while “nearly 75% had contact with primary care providers.” (Luoma et. al.) The conclusion of the study was that prevention “efforts involving primary care may be most effective” in preventing suicide for older generations as well as women, and that it could be a basis for more creative means of reaching out to younger men.
That was the stance from 2002, and yet we don’t see much change in the 14 years since, bringing up the question: Is what we are doing enough?
We live in a society making strides to improvements in the conversation about mental health, but that still has a long way to go. Many people are too uncomfortable to speak out about their feelings, leading to worse and worse symptoms, and in some cases suicide. The medical field is now starting to realize that general physicians have to take a greater role, but it is also up to the average person to reduce the stigma. If a person struggling with depression, anxiety, or some other mental ailment felt that it was socially acceptable for them to speak to someone about their situation, then we may see a reduction in these rates.
With the recent suicide prevention week in mind, we should all take a minute to consider what we can do to reduce the stigma against mental health. It could be as simple as being there for a friend, or having the courage to state our own concerns to the people around us.
This past week here at UConn students observed 1100 flags spread across the lawn in front of the student union, placed in memorial to the average of 1100 college students who commit suicide on college campuses each year. Many took the time to write a message of hope, or one in remembrance of someone whom they had known who committed suicide. It brought it to mind for many people, reminded us that there are people who struggle every day with mental illness, and that there are students like us, who believe they have no other option than to commit suicide.
If one were to stop and talk to the group who were tabling in front of the lawn they would have the opportunity to write their flag, collect a button or a shirt, and maybe pet a dog. But they could also learn a little bit more about the organization behind the event, Active Minds, and its mission to reduce the stigma around mental health. It is generally believed that although an important issue in modern society, there is some sort of disconnect between the people trying to give help and those needing it, partly due to the stigma surrounding admitting to your friends and family that you need help. Regardless, mental health is an issue that general physicians are starting to take more awareness of.
Recently, more and more papers have been published that focused on the ways which primary care physicians, as well as counseling and psychiatry centers, can improve the way in which they approach the issue. Some studies have shown ways to improve the appearance of facilities to make them more friendly, so as to reduce the rates of suicide at in-patient facilities. Others have been published more as advice, based on research, to primary care physicians on how to approach the issue, from simply looking for specific risk factors, to broaching the subject with their patients.
Regardless of who the target audience is, mental health is a topic that needs to be better approached. One study that looked into the medical records of patients who had eventually committed suicide found that “only one third” had spoken to a mental health services center, while “nearly 75% had contact with primary care providers.” (Luoma et. al.) The conclusion of the study was that prevention “efforts involving primary care may be most effective” in preventing suicide for older generations as well as women, and that it could be a basis for more creative means of reaching out to younger men.
That was the stance from 2002, and yet we don’t see much change in the 14 years since, bringing up the question: Is what we are doing enough?
We live in a society making strides to improvements in the conversation about mental health, but that still has a long way to go. Many people are too uncomfortable to speak out about their feelings, leading to worse and worse symptoms, and in some cases suicide. The medical field is now starting to realize that general physicians have to take a greater role, but it is also up to the average person to reduce the stigma. If a person struggling with depression, anxiety, or some other mental ailment felt that it was socially acceptable for them to speak to someone about their situation, then we may see a reduction in these rates.
With the recent suicide prevention week in mind, we should all take a minute to consider what we can do to reduce the stigma against mental health. It could be as simple as being there for a friend, or having the courage to state our own concerns to the people around us.
| Bibliography |
A World Without Eggs
By Shan Kurkcu October 3, 2016
On July 25, 1978, the world witnessed the birth of Louise Joy Brown. Born in Great Britain, Louise was the first baby born via in vitro fertilization. Well, the Brits have yet again defied a long held central dogma. This time the Brits have shown that conception need not be constrained by an egg donor.
Scientist have been able to induce the development of an unfertilized egg into an embryo for quite some time now (parthenogenesis). The first significant breakthrough in parthenogontes, in humans, was at the hands of Dr. Elena Revazova and her team. Dr. Elena Revazova successfully created stem cells from a parthenogenote in 2007. However, Suzuki, T. and his team of Scientists at Bath in england have fertilized a parthenogenote using sperm. Moreover, 24% of the parthenogenotes went on to develop into a healthy mouse pups. This is significant in that it marks the first time development, to term, has been achieved via introducing sperm into an egg which had already begun developing into an embryo. In other words the process of mitosis had already begun with only half the DNA required when the sperm was introduced. The success came in finding that the “programing” of sperm not only occurs at fertilization, but may also occur at the beginning of the first mitotic M-phase. Allowing for a window of time to introduce sperm to a parthenogonte.
“These studies demonstrate that mitotic embryos are able to remodel sperm chromatin completely, leading to the direct production of healthy animals. Full sperm reprogramming is therefore not unique to oocytes, showing that sperm chromatin reprogramming machinery is present at different development stages and in other cell types.”
The team believes that the finding elucidates a possible mechanism in which cells, which have been induced to express pluripotency, may develop into viable embryos which can be carried to term. Prior to these findings it was believed that the biological pathways needed to program a sperm to fertilize an egg lied with in the egg. However, the ability for a cell other than an egg to be fertilized is now a possibility. Dr Perry, a member of the team which performed the research is quoted by Abigeal Beall, in her article as saying “‘we're saying is that these embryos are mitotic cells - mitotic cells are the type of cell that almost every dividing cell in your body is. And therefore, potentially, one day we might be able to extend what we've shown in these mitotic cells to other mitotic cells’”.
In conclusion the implication of these findings may have exciting societal implication. Although further research is needed, this would allow for couples, who do not have to ability to conceive children on their own, to do so. In the field of science, the findings have begun to unravel some of the mystery behind fertilization and development.
On July 25, 1978, the world witnessed the birth of Louise Joy Brown. Born in Great Britain, Louise was the first baby born via in vitro fertilization. Well, the Brits have yet again defied a long held central dogma. This time the Brits have shown that conception need not be constrained by an egg donor.
Scientist have been able to induce the development of an unfertilized egg into an embryo for quite some time now (parthenogenesis). The first significant breakthrough in parthenogontes, in humans, was at the hands of Dr. Elena Revazova and her team. Dr. Elena Revazova successfully created stem cells from a parthenogenote in 2007. However, Suzuki, T. and his team of Scientists at Bath in england have fertilized a parthenogenote using sperm. Moreover, 24% of the parthenogenotes went on to develop into a healthy mouse pups. This is significant in that it marks the first time development, to term, has been achieved via introducing sperm into an egg which had already begun developing into an embryo. In other words the process of mitosis had already begun with only half the DNA required when the sperm was introduced. The success came in finding that the “programing” of sperm not only occurs at fertilization, but may also occur at the beginning of the first mitotic M-phase. Allowing for a window of time to introduce sperm to a parthenogonte.
“These studies demonstrate that mitotic embryos are able to remodel sperm chromatin completely, leading to the direct production of healthy animals. Full sperm reprogramming is therefore not unique to oocytes, showing that sperm chromatin reprogramming machinery is present at different development stages and in other cell types.”
The team believes that the finding elucidates a possible mechanism in which cells, which have been induced to express pluripotency, may develop into viable embryos which can be carried to term. Prior to these findings it was believed that the biological pathways needed to program a sperm to fertilize an egg lied with in the egg. However, the ability for a cell other than an egg to be fertilized is now a possibility. Dr Perry, a member of the team which performed the research is quoted by Abigeal Beall, in her article as saying “‘we're saying is that these embryos are mitotic cells - mitotic cells are the type of cell that almost every dividing cell in your body is. And therefore, potentially, one day we might be able to extend what we've shown in these mitotic cells to other mitotic cells’”.
In conclusion the implication of these findings may have exciting societal implication. Although further research is needed, this would allow for couples, who do not have to ability to conceive children on their own, to do so. In the field of science, the findings have begun to unravel some of the mystery behind fertilization and development.
| Bibliography |
Touching Sensations in Prosthetics
By Zewen Tan October 16, 2016
Prosthetics have been around for over three millennia. Wooden toes attached to a leather casing were dug up in Ancient Egypt recently by archaeologists. In the 16th century, the famous battlefield surgeon Ambroise Pare made a flexible hand with catches and springs as well as a leg that would lock in place so that the user could stand. As warfare advanced, so did the need for amputations and research into improved artificial limbs. The two World Wars saw doctors develop arms so that veterans could return and perform factory and manual labor. In the most recent wars in the Middle East, more than $144 million has been put into development of more functional prosthetics for soldiers suffering from traumatic limb loss.
The money certainly did not go to waste. The i-limb hand from Touch Bionics in 2013 has brought with it a breadth of technological and engineering innovations. Instead of one motor that shuts the hand in a claw grip, each individual finger has smaller motors that allow for a wider range of motion. Pressure sensors are also imbedded in the fingers to prevent the hand from crushing softer objects (ex. Foam cup). Furthermore, instead of a single preset, the i-limb allows software engineers to program each motor specifically to create a variety of configurations in the hand; this adds unprecedented functionality and convenience, as one hand can now perform the actions of the multiple hands that were required in the past. There is even an iPhone/Android app that allows for the user to quickly switch between all of the configurations (1).
While the i-limb has advanced prosthetics more in the last decade than perhaps the last century, it still lacks one crucial function: the sensation of touch. Researchers at the University Of Pittsburgh School Of Medicine are trying to solve this issue right now. Nathan Copeland was left paralyzed below the chest after a car crash in 2004. After implanting two chips into Copeland’s motor cortex as well as two chips in his somatosensory cortex, researchers found that after ten years, Copeland was finally able to feel sensations in the artificial fingers when in contact with another object.
Imaging techniques were used before the implants to determine the exact locations in Copelan’s brain that corresponded with the sense of touch in the hand and arm. This information allowed researchers to reverse program the response of the electrical signals to create sensations in Copeland’s brain. As he describes it himself: “I can feel just about every finger… it’s a really weird sensation. Sometimes it feels electrical and sometimes it’s pressure… It feels like my fingers are getting touched or pushed”. After testing the hand with a cotton swab, senior researcher Robert Gaunt found that Copeland could identify 84% of the time which individual finger was touched while blindfolded (2).
This achievement is will be a harbinger to developing even better senses of touch in prosthetics in the future. As Dr. Vineeta Singh from the UCSF School of medicine describes it, a very specific amount of electrical stimulation is required to imitate the sense of touch. Too much stimulation and the patient can go into shock from pain, while too little stimulation would result in no feeling at all. Much more refinement and improvement is required before a product like this reaches the public market. Not only is it ludicrously expensive right now, but not all the functionality is there yet. Firstly, the hand is not able to create the sensation to differentiate between hot and cold. Furthermore, the pressure technology is also not advanced enough for the patient to formulate an advanced three dimensional image in their mind with depth perception.
Dr. Singh predicts that it would take at least another decade for a prosthetic hand to rival a normal limb in terms of functionality. Achieving the touch sensation is just the first of many steps towards that goal.
Prosthetics have been around for over three millennia. Wooden toes attached to a leather casing were dug up in Ancient Egypt recently by archaeologists. In the 16th century, the famous battlefield surgeon Ambroise Pare made a flexible hand with catches and springs as well as a leg that would lock in place so that the user could stand. As warfare advanced, so did the need for amputations and research into improved artificial limbs. The two World Wars saw doctors develop arms so that veterans could return and perform factory and manual labor. In the most recent wars in the Middle East, more than $144 million has been put into development of more functional prosthetics for soldiers suffering from traumatic limb loss.
The money certainly did not go to waste. The i-limb hand from Touch Bionics in 2013 has brought with it a breadth of technological and engineering innovations. Instead of one motor that shuts the hand in a claw grip, each individual finger has smaller motors that allow for a wider range of motion. Pressure sensors are also imbedded in the fingers to prevent the hand from crushing softer objects (ex. Foam cup). Furthermore, instead of a single preset, the i-limb allows software engineers to program each motor specifically to create a variety of configurations in the hand; this adds unprecedented functionality and convenience, as one hand can now perform the actions of the multiple hands that were required in the past. There is even an iPhone/Android app that allows for the user to quickly switch between all of the configurations (1).
While the i-limb has advanced prosthetics more in the last decade than perhaps the last century, it still lacks one crucial function: the sensation of touch. Researchers at the University Of Pittsburgh School Of Medicine are trying to solve this issue right now. Nathan Copeland was left paralyzed below the chest after a car crash in 2004. After implanting two chips into Copeland’s motor cortex as well as two chips in his somatosensory cortex, researchers found that after ten years, Copeland was finally able to feel sensations in the artificial fingers when in contact with another object.
Imaging techniques were used before the implants to determine the exact locations in Copelan’s brain that corresponded with the sense of touch in the hand and arm. This information allowed researchers to reverse program the response of the electrical signals to create sensations in Copeland’s brain. As he describes it himself: “I can feel just about every finger… it’s a really weird sensation. Sometimes it feels electrical and sometimes it’s pressure… It feels like my fingers are getting touched or pushed”. After testing the hand with a cotton swab, senior researcher Robert Gaunt found that Copeland could identify 84% of the time which individual finger was touched while blindfolded (2).
This achievement is will be a harbinger to developing even better senses of touch in prosthetics in the future. As Dr. Vineeta Singh from the UCSF School of medicine describes it, a very specific amount of electrical stimulation is required to imitate the sense of touch. Too much stimulation and the patient can go into shock from pain, while too little stimulation would result in no feeling at all. Much more refinement and improvement is required before a product like this reaches the public market. Not only is it ludicrously expensive right now, but not all the functionality is there yet. Firstly, the hand is not able to create the sensation to differentiate between hot and cold. Furthermore, the pressure technology is also not advanced enough for the patient to formulate an advanced three dimensional image in their mind with depth perception.
Dr. Singh predicts that it would take at least another decade for a prosthetic hand to rival a normal limb in terms of functionality. Achieving the touch sensation is just the first of many steps towards that goal.
| Bibliography |
Separating the McDonald Twins
By Colin Bixler October 17, 2016
The McDonald twins, Anias and Jadon, were born conjoined at the head, a medical condition referred to as craniopagus twins. At 13 months old, on Thursday October 13, the process began to separate the two boys. Although the boys were mostly healthy, their development was impaired and doctors had concerns about their brain development. Anias had previously had seizures, minor vision problems, and had to be fed through a tube into his stomach. Neither of the boys had the ability to walk or crawl, simply because it was physically impossible for them to do so. As such their parents, Nicole and Christian, had to make the choice to have surgery performed to separate the twins.
The surgeon was Dr. James Goodrich who had performed six previous surgeries separating twins conjoined at the head, out of a mere fifty-nine total surgeries done in the world to date. It’s a very rare condition, requiring very specialized treatment, making it even more difficult and tricky to master.
Dr. Goodrich performed surgery for over twenty hours, by first separating the twins, then having to piece back together each boy’s skull individually and ensure their survival. He was successful, despite the steepness of the task he had at hand.
The survival of Anias and Jadon is a massive medical feat in itself, in addition to being a huge relief and blessing to the McDonald family. In prepping for the surgery Dr. Goodrich and his staff have had to approach new ground at each step. They have crafted anatomically perfect models that map out everything from the shape of the twin’s head, to a map of every blood vessel within their small brains. Even then, they still didn’t truly know what they would find when they got into surgery.
The most shocking part of this isn’t necessarily the separation itself, it’s the knowledge that a team of surgeons, nurses, and specialists can even begin to approach the issue. In the past it was widely accepted by the medical community for the surgeon to do his absolute best to simply save one twin. It was considered impossible for both to survive, and if somehow they did it would be with one of the two having severe mental impairments. Death and/or mental disability was expected, unimpaired survival was not. Some of the techniques and equipment used in the McDonald’s surgery has never been used before in a surgery, even one of Dr. Goodrich’s previous six separations.
That’s not to say that the boys are out of the woods yet. There are still months of rehabilitation that have to occur and nothing is certain that they will come out unscathed. But it’s astonishing that medicine has reached a point where successes like this are a possibility, and not some fantasy. Medicine has experienced a technological revolution that is probably one of the major reasons the boys were successfully separated. 3-D scanning revealed the inner workings of the twin’s joined heads. Biomedical engineers working in Colorado were able to edit these images, in whatever way the surgeons desired, while simultaneously streaming them to the conference room for the team back in New York. In addition models were crafted for how to deal with each aspect of the boys’ brains. The whole process is a medical marvel.
Aside from technological revolution, there is a vast network within medicine making it possible for experts from all over the world to work together. Countries, hospitals, and doctors are all interconnected, and becoming more so each day. Medicine is at an all time high that has never been seen before.
It’s an exciting world out there for people within the medical industry. New developments are happening every day, making surgeries that are almost unimaginably intricate like the McDonald twins’ even more likely to end in success.
The McDonald twins, Anias and Jadon, were born conjoined at the head, a medical condition referred to as craniopagus twins. At 13 months old, on Thursday October 13, the process began to separate the two boys. Although the boys were mostly healthy, their development was impaired and doctors had concerns about their brain development. Anias had previously had seizures, minor vision problems, and had to be fed through a tube into his stomach. Neither of the boys had the ability to walk or crawl, simply because it was physically impossible for them to do so. As such their parents, Nicole and Christian, had to make the choice to have surgery performed to separate the twins.
The surgeon was Dr. James Goodrich who had performed six previous surgeries separating twins conjoined at the head, out of a mere fifty-nine total surgeries done in the world to date. It’s a very rare condition, requiring very specialized treatment, making it even more difficult and tricky to master.
Dr. Goodrich performed surgery for over twenty hours, by first separating the twins, then having to piece back together each boy’s skull individually and ensure their survival. He was successful, despite the steepness of the task he had at hand.
The survival of Anias and Jadon is a massive medical feat in itself, in addition to being a huge relief and blessing to the McDonald family. In prepping for the surgery Dr. Goodrich and his staff have had to approach new ground at each step. They have crafted anatomically perfect models that map out everything from the shape of the twin’s head, to a map of every blood vessel within their small brains. Even then, they still didn’t truly know what they would find when they got into surgery.
The most shocking part of this isn’t necessarily the separation itself, it’s the knowledge that a team of surgeons, nurses, and specialists can even begin to approach the issue. In the past it was widely accepted by the medical community for the surgeon to do his absolute best to simply save one twin. It was considered impossible for both to survive, and if somehow they did it would be with one of the two having severe mental impairments. Death and/or mental disability was expected, unimpaired survival was not. Some of the techniques and equipment used in the McDonald’s surgery has never been used before in a surgery, even one of Dr. Goodrich’s previous six separations.
That’s not to say that the boys are out of the woods yet. There are still months of rehabilitation that have to occur and nothing is certain that they will come out unscathed. But it’s astonishing that medicine has reached a point where successes like this are a possibility, and not some fantasy. Medicine has experienced a technological revolution that is probably one of the major reasons the boys were successfully separated. 3-D scanning revealed the inner workings of the twin’s joined heads. Biomedical engineers working in Colorado were able to edit these images, in whatever way the surgeons desired, while simultaneously streaming them to the conference room for the team back in New York. In addition models were crafted for how to deal with each aspect of the boys’ brains. The whole process is a medical marvel.
Aside from technological revolution, there is a vast network within medicine making it possible for experts from all over the world to work together. Countries, hospitals, and doctors are all interconnected, and becoming more so each day. Medicine is at an all time high that has never been seen before.
It’s an exciting world out there for people within the medical industry. New developments are happening every day, making surgeries that are almost unimaginably intricate like the McDonald twins’ even more likely to end in success.
| Bibliography |
Athletes to Amnesia: Youth Concussions
By Anneliese Lapides October 16, 2016
Sports are extremely popular among the youth in America: basketball, baseball, soccer, and football are among the most favored and have the most participants1. Contact sports, such as football, pose the risk of different injuries, one of the most serious concussions. Concussions are traumatic brain injuries caused by impact to the head. The brain is protected from outside dangers by the skull; the brain is also surrounded by spinal fluid that acts as a cushion between the organ and the skull2. When a person’s head, or even body, is hit with extreme force, the spinal fluid can be an inadequate protective measure in comparison to the force of the trauma – thus causing a concussion. There may be no physical signs of a concussion, but symptoms include headaches, concentration issues, dizziness, and more extreme medical issues in some situations2. Scientists and medical professionals are starting to record a large increase in the amount of concussions amongst the youth in America, and they are starting to note the possible long-term and developmental effects on those who suffer from concussion earlier on in their lives.
According to medical data collected by Blue Cross Blue Shield, there has been a 71% increase in contact-sport related concussion among American youth, ages 10-19, since 20103. They also noted that the majority of youth concussion patients are diagnosed in the fall, during football, soccer, and rugby season3. The data also showed that athletes ages 10-19 are five times more likely than any other age group to suffer from concussions3. Not only are athletes in this young age range more likely to be diagnosed with concussions, but it also more likely for them to suffer from multiple concussions because of continued participation in physical activity, possibly without diagnosis of the first concussion. Since this brain injury can be invisible to the naked eye and symptoms may be minor or not prevalent, young athletes are faced with a risk of suffering traumatic brain damage.
Medical professionals, not just in the United States, are noticing that there is a chance of long-term effects due to concussions. Dr. Maryse Lassonde, a Canadian neuropsychologist studied the effects of recurring head trauma on athletes of different ages4. In her most current research, Dr. Lassonde compared the neurological health of people who had suffered concussions about 30 years ago to individuals who have never had a concussion. Her results showed that those who experienced concussions at some point in their lifetime, even as far back as 30 years ago, experienced symptoms similar to those of Parkinson’s Disease (i.e. motor problems, attention problems, memory loss)4. Dr. Lassonde also observed brain thinning in the athletes who have experienced concussions over their lifetimes, which is usually seen in Alzheimer’s patients and is associated with memory loss. Lastly, she noted that some of the athletes suffered from chronic traumatic encephalopathy (CTE) – a condition caused by “repeated blows to the head”5. CTE is a form of chronic brain damage that has been found in the brains of many former athletes, such as retired football players, and can cause dementia and personality disorders5.
Medical research is showing a trend in the detrimental long-term health effects of athletes who have suffered multiple concussions from participating in [contact] sports over their lifetime or as kids/teenagers. This calls into question what can be done to prevent this type of brain trauma from occurring so frequently. The rate at which concussion diagnosis among young athletes is increasing also presents an opportunity for health care professionals to possibly develop cures for this type of brain damage, or find ways to reverse the effects concussions have on the brain. Youth sports are becoming more and more popular throughout the country, meaning that this is an issue that should strongly be looked into. Research in preventative or curative medicine for youth concussions would help to provide the most safety for children while they play the sports they love. In addition, taking action to reduce the amount of youth concussions could allow kids and teenagers to continue to play these sports without having to fear what health detriments they could face in the future.
Sports are extremely popular among the youth in America: basketball, baseball, soccer, and football are among the most favored and have the most participants1. Contact sports, such as football, pose the risk of different injuries, one of the most serious concussions. Concussions are traumatic brain injuries caused by impact to the head. The brain is protected from outside dangers by the skull; the brain is also surrounded by spinal fluid that acts as a cushion between the organ and the skull2. When a person’s head, or even body, is hit with extreme force, the spinal fluid can be an inadequate protective measure in comparison to the force of the trauma – thus causing a concussion. There may be no physical signs of a concussion, but symptoms include headaches, concentration issues, dizziness, and more extreme medical issues in some situations2. Scientists and medical professionals are starting to record a large increase in the amount of concussions amongst the youth in America, and they are starting to note the possible long-term and developmental effects on those who suffer from concussion earlier on in their lives.
According to medical data collected by Blue Cross Blue Shield, there has been a 71% increase in contact-sport related concussion among American youth, ages 10-19, since 20103. They also noted that the majority of youth concussion patients are diagnosed in the fall, during football, soccer, and rugby season3. The data also showed that athletes ages 10-19 are five times more likely than any other age group to suffer from concussions3. Not only are athletes in this young age range more likely to be diagnosed with concussions, but it also more likely for them to suffer from multiple concussions because of continued participation in physical activity, possibly without diagnosis of the first concussion. Since this brain injury can be invisible to the naked eye and symptoms may be minor or not prevalent, young athletes are faced with a risk of suffering traumatic brain damage.
Medical professionals, not just in the United States, are noticing that there is a chance of long-term effects due to concussions. Dr. Maryse Lassonde, a Canadian neuropsychologist studied the effects of recurring head trauma on athletes of different ages4. In her most current research, Dr. Lassonde compared the neurological health of people who had suffered concussions about 30 years ago to individuals who have never had a concussion. Her results showed that those who experienced concussions at some point in their lifetime, even as far back as 30 years ago, experienced symptoms similar to those of Parkinson’s Disease (i.e. motor problems, attention problems, memory loss)4. Dr. Lassonde also observed brain thinning in the athletes who have experienced concussions over their lifetimes, which is usually seen in Alzheimer’s patients and is associated with memory loss. Lastly, she noted that some of the athletes suffered from chronic traumatic encephalopathy (CTE) – a condition caused by “repeated blows to the head”5. CTE is a form of chronic brain damage that has been found in the brains of many former athletes, such as retired football players, and can cause dementia and personality disorders5.
Medical research is showing a trend in the detrimental long-term health effects of athletes who have suffered multiple concussions from participating in [contact] sports over their lifetime or as kids/teenagers. This calls into question what can be done to prevent this type of brain trauma from occurring so frequently. The rate at which concussion diagnosis among young athletes is increasing also presents an opportunity for health care professionals to possibly develop cures for this type of brain damage, or find ways to reverse the effects concussions have on the brain. Youth sports are becoming more and more popular throughout the country, meaning that this is an issue that should strongly be looked into. Research in preventative or curative medicine for youth concussions would help to provide the most safety for children while they play the sports they love. In addition, taking action to reduce the amount of youth concussions could allow kids and teenagers to continue to play these sports without having to fear what health detriments they could face in the future.
| Bibliography |
New Study Shows Why Women Are More Susceptible to Eating Disorders
By Meghan Goddard October 17, 2016
Statistics have shown that body dissatisfaction and eating disorders are more common in women than men. Scientists and nutritionists have wondered if this is due to certain societal pressures, some biological component, or a combination of both. The Department of Psychology at York University in the UK recently published a study showing that women actually show increased brain activity related to negative body perception over men (Whiteman).
NEDA, National Eating Disorder Association, reports that in the U.S., there are 20 million women compared to 10 million men, suffering from clinically significant eating disorders at some point in their lifetimes. These eating disorders include anorexia nervosa, bulimia nervosa, binge eating disorder, and other specified feeding or eating disorder, but only those reported and registered in a clinic. This does not include those going undiagnosed. Eating disorders have been linked to mortality, especially high suicide rates (National Eating Disorder Association).
Dr. Catherine Preston of the York University study believes body dissatisfaction is an underlying factor effecting high rates of eating disorders in women. The study showed that society does contributes to how both men and women negatively perceive themselves. Preston believes women are more susceptible to these social pressures (Whiteman). With media displaying women to want to look a certain way, and dieting industries taking over the advertising world, these social pressures seem inescapable.
Because there is so little research on the biological predispositions to eating disorders, Dr. Preston and colleagues conducted a study to test neural activity associated with negative body perception. The study consisted of participants with no history of eating disorders. Sixteen men and sixteen women participants wore a virtual reality headset. This headset made it appear as if they had a specific body shape. Participants were poked with a stick at the same time it was shown the virtual body was. This helped to better perceive the virtual display as their own body. This was done for different versions of slim and obese body types. While they looked at and processed their “new bodies” their brain activity was measured via MRI (Whiteman).
The results supported Dr. Preston’s hypothesis. When both the men and women observed their virtual bodies, brain activity was seen in the parietal lobe. This lobe has an association area of body perception. Activity was also seen in the anterior cingulate cortex (Whiteman). This brain region is in connection with the limbic system and prefrontal cortex, meaning it relates to both the emotional and cognitive integration. It has been seen to relate to maladaptive behaviors to control and regulate painful emotions. This often results in motivation toward negative behaviors, including substance abuse, suicide, and eating disorders as coping mechanisms to these emotions (Hurley, et al.). As hypothesized, they found that this brain activity was more prominent in women than in men. This can be interpreted to show that women have more body dissatisfaction when they were perceived to have an obese body, than in men. Not only does the study show links between gender and body perception, but also shows why often our emotional responses regarding these emotions are harmful (Whiteman).
Although this is interesting in showing neural responses, I don’t think it shows that body perception is entirely biological. Our social perceptions may be what causes us to associate obese bodies with negative emotions. As someone who has followed studies in eating disorders and body confidence in young women, I believe social aspects have the biggest negative influence on body perception. When women have social standards to have a certain body shape and act confident, it creates this ideal, unreachable image and looks down on anything but it. This perception of the ideal woman mixed with parts of the brain that link negative response to these emotions, can result in deadly consequences. This is something to be cautious about and know when to recognize signs of eating disorders in family and friends. The more we learn about these disorders, the more I hope we can help people from suffering. More than twice the amount of women may be suffering, but 10 million men is still a huge number. Dr. Patterson says they are performing further research on eating disorder’s effect on women (Whiteman). Hopefully this will lead to a way to scientifically decrease these negative perceptions in both men and women. In the meantime, we can do the most we can to sway society from creating this ideal body image and learn to help those who need it.
Statistics have shown that body dissatisfaction and eating disorders are more common in women than men. Scientists and nutritionists have wondered if this is due to certain societal pressures, some biological component, or a combination of both. The Department of Psychology at York University in the UK recently published a study showing that women actually show increased brain activity related to negative body perception over men (Whiteman).
NEDA, National Eating Disorder Association, reports that in the U.S., there are 20 million women compared to 10 million men, suffering from clinically significant eating disorders at some point in their lifetimes. These eating disorders include anorexia nervosa, bulimia nervosa, binge eating disorder, and other specified feeding or eating disorder, but only those reported and registered in a clinic. This does not include those going undiagnosed. Eating disorders have been linked to mortality, especially high suicide rates (National Eating Disorder Association).
Dr. Catherine Preston of the York University study believes body dissatisfaction is an underlying factor effecting high rates of eating disorders in women. The study showed that society does contributes to how both men and women negatively perceive themselves. Preston believes women are more susceptible to these social pressures (Whiteman). With media displaying women to want to look a certain way, and dieting industries taking over the advertising world, these social pressures seem inescapable.
Because there is so little research on the biological predispositions to eating disorders, Dr. Preston and colleagues conducted a study to test neural activity associated with negative body perception. The study consisted of participants with no history of eating disorders. Sixteen men and sixteen women participants wore a virtual reality headset. This headset made it appear as if they had a specific body shape. Participants were poked with a stick at the same time it was shown the virtual body was. This helped to better perceive the virtual display as their own body. This was done for different versions of slim and obese body types. While they looked at and processed their “new bodies” their brain activity was measured via MRI (Whiteman).
The results supported Dr. Preston’s hypothesis. When both the men and women observed their virtual bodies, brain activity was seen in the parietal lobe. This lobe has an association area of body perception. Activity was also seen in the anterior cingulate cortex (Whiteman). This brain region is in connection with the limbic system and prefrontal cortex, meaning it relates to both the emotional and cognitive integration. It has been seen to relate to maladaptive behaviors to control and regulate painful emotions. This often results in motivation toward negative behaviors, including substance abuse, suicide, and eating disorders as coping mechanisms to these emotions (Hurley, et al.). As hypothesized, they found that this brain activity was more prominent in women than in men. This can be interpreted to show that women have more body dissatisfaction when they were perceived to have an obese body, than in men. Not only does the study show links between gender and body perception, but also shows why often our emotional responses regarding these emotions are harmful (Whiteman).
Although this is interesting in showing neural responses, I don’t think it shows that body perception is entirely biological. Our social perceptions may be what causes us to associate obese bodies with negative emotions. As someone who has followed studies in eating disorders and body confidence in young women, I believe social aspects have the biggest negative influence on body perception. When women have social standards to have a certain body shape and act confident, it creates this ideal, unreachable image and looks down on anything but it. This perception of the ideal woman mixed with parts of the brain that link negative response to these emotions, can result in deadly consequences. This is something to be cautious about and know when to recognize signs of eating disorders in family and friends. The more we learn about these disorders, the more I hope we can help people from suffering. More than twice the amount of women may be suffering, but 10 million men is still a huge number. Dr. Patterson says they are performing further research on eating disorder’s effect on women (Whiteman). Hopefully this will lead to a way to scientifically decrease these negative perceptions in both men and women. In the meantime, we can do the most we can to sway society from creating this ideal body image and learn to help those who need it.
| Bibliography |
The Newest Advancements In Immunotherapy
By Anneliese Lapides October 31, 2016
Immunotherapy is a certain type of treatment that is being highly investigated by doctors and oncologists in the battle against cancer. Immunotherapy is an alternative treatment that uses a patient’s own immune system to fight cancer1. Many people think of radiation or chemotherapy when thinking of methods to treat cancer; current developments being made in the search for a cure have paved the way for immunotherapy to become another highly sought out remedy.
There are different types of immunotherapy, including monoclonal antibodies, immune checkpoint inhibitors, and cancer vaccines. Monoclonal antibodies are synthetic immune system proteins. The man-made antibodies are designed to attack specific parts of cancer cells in order to kill them efficiently and quickly1. Immune checkpoint inhibitors are drugs that encourage the immune system to recognize foreign, cancerous cells and attack them1. Lastly, cancer vaccines are another form of immunotherapy. The vaccine would contain a substance that would trigger an immune response to the presence of cancerous cells1. Cancer vaccines could be used to prevent cancer from further developing in the body, as well as be used for preventative measures.
“The father of cancer immunotherapy” was Dr. William Coley, a doctor who studied sarcoma in a woman named Bessie in the 1890s2. Dr. Coley created a bacterial cocktail in order to create a man-made infection to act as a vaccine2. The bacterial cocktail would cause a patient’s body to initiate an immune response and recognize that the malignant tumors were an invasive, foreign body. The immune system would then attack the cancerous cells.
The most recent advancement in immunotherapy cancer treatments is the FDA’s approval of the immunotherapy drug KEYTRUDA. KEYTRUDA is meant to initiate an immune response in order to help treat patients with “metastatic non-small-cell lung cancer”2. This drug is the only immunotherapy drug that the FDA has approved for first-line cancer treatment2. First-line cancer treatment means that the drug or method is used as the initial/first treatment given to a patient3.
There are risks associated with immunotherapy drugs such as KEYTRUDA, as there are risks with all medicine. While immunotherapy drugs help use the immune system’s natural function to fight against cancer, the medicine can also affect the system in a way that causes it to attack regularly functioning organs and tissues in the body4. Even though there is risk involved, doctors can use drugs like KEYTRUDA as the first step in finally solving the mystery of how to cure cancer for good. A benefit to the drug is that it helps fight advanced cancers; this is a sign that the immunotherapy treatments being developed are not only able to help prevent cancer development and metastasis, but they can also help save the lives of patients whose cancer has been detected in later stages. These developments demonstrate a positive outlook into the future of cancer treatment, and the possibility of immunotherapy at the forefront of this research.
Immunotherapy is a certain type of treatment that is being highly investigated by doctors and oncologists in the battle against cancer. Immunotherapy is an alternative treatment that uses a patient’s own immune system to fight cancer1. Many people think of radiation or chemotherapy when thinking of methods to treat cancer; current developments being made in the search for a cure have paved the way for immunotherapy to become another highly sought out remedy.
There are different types of immunotherapy, including monoclonal antibodies, immune checkpoint inhibitors, and cancer vaccines. Monoclonal antibodies are synthetic immune system proteins. The man-made antibodies are designed to attack specific parts of cancer cells in order to kill them efficiently and quickly1. Immune checkpoint inhibitors are drugs that encourage the immune system to recognize foreign, cancerous cells and attack them1. Lastly, cancer vaccines are another form of immunotherapy. The vaccine would contain a substance that would trigger an immune response to the presence of cancerous cells1. Cancer vaccines could be used to prevent cancer from further developing in the body, as well as be used for preventative measures.
“The father of cancer immunotherapy” was Dr. William Coley, a doctor who studied sarcoma in a woman named Bessie in the 1890s2. Dr. Coley created a bacterial cocktail in order to create a man-made infection to act as a vaccine2. The bacterial cocktail would cause a patient’s body to initiate an immune response and recognize that the malignant tumors were an invasive, foreign body. The immune system would then attack the cancerous cells.
The most recent advancement in immunotherapy cancer treatments is the FDA’s approval of the immunotherapy drug KEYTRUDA. KEYTRUDA is meant to initiate an immune response in order to help treat patients with “metastatic non-small-cell lung cancer”2. This drug is the only immunotherapy drug that the FDA has approved for first-line cancer treatment2. First-line cancer treatment means that the drug or method is used as the initial/first treatment given to a patient3.
There are risks associated with immunotherapy drugs such as KEYTRUDA, as there are risks with all medicine. While immunotherapy drugs help use the immune system’s natural function to fight against cancer, the medicine can also affect the system in a way that causes it to attack regularly functioning organs and tissues in the body4. Even though there is risk involved, doctors can use drugs like KEYTRUDA as the first step in finally solving the mystery of how to cure cancer for good. A benefit to the drug is that it helps fight advanced cancers; this is a sign that the immunotherapy treatments being developed are not only able to help prevent cancer development and metastasis, but they can also help save the lives of patients whose cancer has been detected in later stages. These developments demonstrate a positive outlook into the future of cancer treatment, and the possibility of immunotherapy at the forefront of this research.
| Bibliography |
Medicine in Mosul
By Colin Bixler October 30, 2016
As the military offensive to retake Mosul grows nearer more and more humanitarian agencies are pressuring governments to increase the amount of medical aid is being sent to the area for civilians, as well as setting up more refugee camps. There is not much known about the medical situation in Mosul, but it is expected that there will be a large outflow of civilians as the battle progresses and that many of them will require immediate medical help.
According to a press release by the International Medical Corps, there are about 1.2 million people already displaced in the area around Mosul and that “hundreds of thousands of additional people could flee Mosul” as the offensive progresses. This poses a serious need for the international community to provide medical assistance both in the form of treatments as simply providing shelter for the refugees.
Already many countries have promised to increase money flowing into the refugee effort to accommodate the influx. The UK pledged 14 million pounds to the effort, for the purpose of improving living conditions by setting up temporary housing as well as providing medical care and physicians to the refugees. Australia announced that it was going to send another 7.6 million on top of the already 46 million they have provided since 2014. The US pledged back in September to provide another 181 million to Iraq in aid as well.
There isn’t much known about the condition of the health care system in Mosul at the moment. What is known however comes from the doctors, nurses, and care providers inside the city, as reported by Niqash an agency that reports on events occurring in Iraq. What is known is that the medical system has been becoming worse and worse as the incursion continues. There are no vaccines for children, very little opportunity for people needing operations or treatments to get it in a timely manner. The costs of treatment are about what they are across Iraq, but the people in the city have no money to pay for them because of a lack of work. Also the funding being provided to the hospitals is estimated to be only a third of what it is supposed to be, as the rest is confiscated by ISIS.
There are also reports coming out that members of ISIS as well as their families are given preferential treatment. Doctors are unable to refuse treatment to them and often are forced to provide it free of charge. This cuts into the ability of civilians not aligned with the group to suffer due to lack of availability. Because of the decreased funding, doctors are earning less money and are losing money when they provide free services to the fighters. In addition because the hospitals have so little funding to work with they are unable to get the necessary medical supplies.
Many humanitarian agencies are fearful that when the offensive finally does
reach the city there will be a large portion of civilians in need of immediate medical attention, because the fighting may result in injuries to them. For the international community to help out the expected hundreds of thousands of refugees that will be fleeing the city in the coming weeks, they need to ensure that there is plenty of support in place, including shelter, basic necessities, food and water, medicine, and medical care in the form of doctors and nurses.
As the military offensive to retake Mosul grows nearer more and more humanitarian agencies are pressuring governments to increase the amount of medical aid is being sent to the area for civilians, as well as setting up more refugee camps. There is not much known about the medical situation in Mosul, but it is expected that there will be a large outflow of civilians as the battle progresses and that many of them will require immediate medical help.
According to a press release by the International Medical Corps, there are about 1.2 million people already displaced in the area around Mosul and that “hundreds of thousands of additional people could flee Mosul” as the offensive progresses. This poses a serious need for the international community to provide medical assistance both in the form of treatments as simply providing shelter for the refugees.
Already many countries have promised to increase money flowing into the refugee effort to accommodate the influx. The UK pledged 14 million pounds to the effort, for the purpose of improving living conditions by setting up temporary housing as well as providing medical care and physicians to the refugees. Australia announced that it was going to send another 7.6 million on top of the already 46 million they have provided since 2014. The US pledged back in September to provide another 181 million to Iraq in aid as well.
There isn’t much known about the condition of the health care system in Mosul at the moment. What is known however comes from the doctors, nurses, and care providers inside the city, as reported by Niqash an agency that reports on events occurring in Iraq. What is known is that the medical system has been becoming worse and worse as the incursion continues. There are no vaccines for children, very little opportunity for people needing operations or treatments to get it in a timely manner. The costs of treatment are about what they are across Iraq, but the people in the city have no money to pay for them because of a lack of work. Also the funding being provided to the hospitals is estimated to be only a third of what it is supposed to be, as the rest is confiscated by ISIS.
There are also reports coming out that members of ISIS as well as their families are given preferential treatment. Doctors are unable to refuse treatment to them and often are forced to provide it free of charge. This cuts into the ability of civilians not aligned with the group to suffer due to lack of availability. Because of the decreased funding, doctors are earning less money and are losing money when they provide free services to the fighters. In addition because the hospitals have so little funding to work with they are unable to get the necessary medical supplies.
Many humanitarian agencies are fearful that when the offensive finally does
reach the city there will be a large portion of civilians in need of immediate medical attention, because the fighting may result in injuries to them. For the international community to help out the expected hundreds of thousands of refugees that will be fleeing the city in the coming weeks, they need to ensure that there is plenty of support in place, including shelter, basic necessities, food and water, medicine, and medical care in the form of doctors and nurses.
| Bibliography |
Stress: The Steady Killer
By Meghan Goddard October 31, 2016
One factor all humans are forced to deal with is stress. Stress sets us apart from most other species. Humans have the highest rate of stress related diseases (Goudarzi). Many modern and prevalent diseases are caused or worsened by stress, such as Alzheimer’s, heart disease, high blood pressure, flu virus, and diabetes. Even in a physically active occupation, stress can negate the benefits of the exercise. These diseases caused by stress are consistent throughout variations in age, sex, BMI, and exercise, proving it is an issue us effecting all (Bryner).
A study on Israeli workers from 1998 to 2003 tested the subjects on job burnout, which is a state of emotional, physical, or mental exhaustion associated with workplace followed by feelings of incompetence and lack of value in one’s work (Mayo clinic). The study found half of their sample of 677 workers of mixed occupations, and mixed levels of control in the workplace, had developed burnout. Of those, 17 had developed Type 2 diabetes in those five years, which is 3.2% of the burnout workers. Researchers believe stress triggers factors of diabetes such as a decrease in necessary cholesterol, along with a large increase in fatty acids in the blood (Bryner). Stress can also be detrimental by the unhealthy behaviors we carryout to cope with different life stressors. Often poor eating habits, drinking alcohol, smoking cigarettes, having a sedentary life style, etc. are used to cope with stress (Dotinga). These can also lead to illnesses like diabetes and cancer. Stress in general can disturb the body’s glucose production, one of the most important processes in the human body (Bryner). All of which can be damaging to our physical health.
A study at Indiana University found that low control in a stressful workplace correlates with stress related disease and even death. Essentially, the less control one has, the younger they die. Comparably, those in high demand jobs who did have high control, decreased their chances of death during the study by 34%. A study at Wisconsin also showed that a higher percentage of workers with less control over their stress provoking jobs are overweight. This is compared to those in control of setting their own goals and make their own decisions on executing and prioritizing work. The low control jobs were those of less power, such as construction workers, mechanics, and nursing aids, while the high-control jobs were mostly supervisors, inspectors, and craftsmen. In this study, the low control had a 15.4% higher likelihood of death compared to the high control. Critiques of this study say these high control jobs tend to come with more responsibility and therefore are more stressful. However, Dr. Gonzalez-Mule argues that this is a different form of stress. The pressure to work fast and concentrate, in fact results in feelings of accomplishment. Joshua Klapow, a clinical psychologist at the University of Alabama, claims it is not about the pressure of amount of work or difficulty of work, but the actual control the employee has over outcomes and decisions. They suggest employees setting their own schedules may reduce this stress in the workplace (Dotinga).
These articles fail to go into deep detail about mental health. There is no doubt that stress can affect one’s mentality. It can lead to depression, anxiety, and other mental illnesses. This is something unique to primates. Stanford University neuroscientist, Robert Sapolsky does however mention that although as a species we struggle most with feelings of stress, we often have positive coping methods that no other animal can experience. He makes an inspiring point, that
“…there's no primate out there that can feel better in life just by listening to Beethoven”
We are able to find comfort through outlets and others that other animals lack. Feelings of connection and knowing other people feel as we do, reduces stress and is unique to humans (Goudarzi).
Although most studies revolve around stress from the workplace, students deal with a great deal of stress themselves. Most of us have never met a college student who said they were not stressed. Exams, deadlines, extracurricular activities, GPAs, debt, maintaining a social life, forming relationships, and all other stressors could be cutting time off of our lives as university students as well. This is a positive reminder to work toward your career goals in doing something you love that will not stress you out for the rest of your life. Be the doctors, nurses, lawyers, artists, CEOs, teachers, and engineers that we are all stressing out trying to be, so you can have your control and enjoy your life to avoid burnout. It is also important to keep in mind while working our way to these positions, that there needs to be a healthy outlet. Joining a club that you genuinely enjoy or find a hobby you can continue with when your future career gets too stressful and your boss is too controlling as an outlet. This can avoid diseases associated with stress, but also unhealthy habits that typically result from it.
One factor all humans are forced to deal with is stress. Stress sets us apart from most other species. Humans have the highest rate of stress related diseases (Goudarzi). Many modern and prevalent diseases are caused or worsened by stress, such as Alzheimer’s, heart disease, high blood pressure, flu virus, and diabetes. Even in a physically active occupation, stress can negate the benefits of the exercise. These diseases caused by stress are consistent throughout variations in age, sex, BMI, and exercise, proving it is an issue us effecting all (Bryner).
A study on Israeli workers from 1998 to 2003 tested the subjects on job burnout, which is a state of emotional, physical, or mental exhaustion associated with workplace followed by feelings of incompetence and lack of value in one’s work (Mayo clinic). The study found half of their sample of 677 workers of mixed occupations, and mixed levels of control in the workplace, had developed burnout. Of those, 17 had developed Type 2 diabetes in those five years, which is 3.2% of the burnout workers. Researchers believe stress triggers factors of diabetes such as a decrease in necessary cholesterol, along with a large increase in fatty acids in the blood (Bryner). Stress can also be detrimental by the unhealthy behaviors we carryout to cope with different life stressors. Often poor eating habits, drinking alcohol, smoking cigarettes, having a sedentary life style, etc. are used to cope with stress (Dotinga). These can also lead to illnesses like diabetes and cancer. Stress in general can disturb the body’s glucose production, one of the most important processes in the human body (Bryner). All of which can be damaging to our physical health.
A study at Indiana University found that low control in a stressful workplace correlates with stress related disease and even death. Essentially, the less control one has, the younger they die. Comparably, those in high demand jobs who did have high control, decreased their chances of death during the study by 34%. A study at Wisconsin also showed that a higher percentage of workers with less control over their stress provoking jobs are overweight. This is compared to those in control of setting their own goals and make their own decisions on executing and prioritizing work. The low control jobs were those of less power, such as construction workers, mechanics, and nursing aids, while the high-control jobs were mostly supervisors, inspectors, and craftsmen. In this study, the low control had a 15.4% higher likelihood of death compared to the high control. Critiques of this study say these high control jobs tend to come with more responsibility and therefore are more stressful. However, Dr. Gonzalez-Mule argues that this is a different form of stress. The pressure to work fast and concentrate, in fact results in feelings of accomplishment. Joshua Klapow, a clinical psychologist at the University of Alabama, claims it is not about the pressure of amount of work or difficulty of work, but the actual control the employee has over outcomes and decisions. They suggest employees setting their own schedules may reduce this stress in the workplace (Dotinga).
These articles fail to go into deep detail about mental health. There is no doubt that stress can affect one’s mentality. It can lead to depression, anxiety, and other mental illnesses. This is something unique to primates. Stanford University neuroscientist, Robert Sapolsky does however mention that although as a species we struggle most with feelings of stress, we often have positive coping methods that no other animal can experience. He makes an inspiring point, that
“…there's no primate out there that can feel better in life just by listening to Beethoven”
We are able to find comfort through outlets and others that other animals lack. Feelings of connection and knowing other people feel as we do, reduces stress and is unique to humans (Goudarzi).
Although most studies revolve around stress from the workplace, students deal with a great deal of stress themselves. Most of us have never met a college student who said they were not stressed. Exams, deadlines, extracurricular activities, GPAs, debt, maintaining a social life, forming relationships, and all other stressors could be cutting time off of our lives as university students as well. This is a positive reminder to work toward your career goals in doing something you love that will not stress you out for the rest of your life. Be the doctors, nurses, lawyers, artists, CEOs, teachers, and engineers that we are all stressing out trying to be, so you can have your control and enjoy your life to avoid burnout. It is also important to keep in mind while working our way to these positions, that there needs to be a healthy outlet. Joining a club that you genuinely enjoy or find a hobby you can continue with when your future career gets too stressful and your boss is too controlling as an outlet. This can avoid diseases associated with stress, but also unhealthy habits that typically result from it.
| Bibliography |
